All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional.
The SOT Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the SOT Hub cannot guarantee the accuracy of translated content. The SOT Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.

The Solid Organ Transplant is an independent medical education platform, sponsored by Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View solid organ transplantation content recommended for you
Preventing complications in SOT: The role of ECP in inducing immune tolerance
Do you know... Which of the following best describes the primary mechanism by which ECP promotes immune tolerance in SOT recipients?
Solid organ transplantation is an established, life-saving or life-prolonging therapeutic intervention for patients with end-stage organ failure or severe organ damage that markedly diminishes quality of life.1,2 In 2025, 49,065 patients in the US and 7,967 patients in Europe received a solid organ transplant (SOT).3,4 While SOT practices continue to evolve, graft loss due to immune rejection remains a critical post-transplant complication.1,2
Immunological mechanisms of SOT rejection
Transplant rejection is modulated via innate and adaptive immune responses and can be classified as acute or chronic, and as T cell- or B cell-mediated, although mixed rejection types have been reported.2,5 The innate immune response is guided by neutrophils, macrophages, natural killer cells, and dendritic cells, which activate adaptive immune responses and cause graft damage through the release of reactive oxygen species and pro-inflammatory cytokines.5 The adaptive immune response depends on T cells, which further stimulate the innate immune response, activate B cells, and cause direct damage through pro-apoptotic enzymes; and B cells, which differentiate into plasma and memory B cells and induce antibody-dependent cell-mediated cytotoxicity.6
Immune tolerance as a therapeutic goal in solid organ transplantation
To circumvent graft rejection, systemic, life-long immunosuppressive regimens are usually administered, including induction, maintenance, and rejection protocols, with the ultimate goal of suppressing the innate and adaptive immune responses.1 While improvements in short-term graft survival have been observed, current immunosuppressive strategies do not promote long-term graft survival.5 Systemic immunosuppression is also associated with an increased risk of infection, metabolic derangements, and various malignancies.1 There is therefore a need for better comprehension and promotion of the mechanisms that determine SOT tolerance, as well as for agents that provide immunomodulation rather than immunosuppression, in order to improve patient outcomes.2,5,7,8
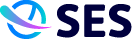
Immune tolerance in solid organ transplantation refers to a state in which a transplant recipient’s immune system accepts a transplanted organ without mounting destructive alloimmune responses.8 Immune tolerance can be separated into central and peripheral tolerance (Figure 1).8
Figure 1. Central and peripheral immune tolerance mechanisms
Central tolerance mechanisms occur in the primary lymphoid organs (bone marrow and thymus), where autoreactive lymphocytes are selectively prevented from entering the secondary lymphoid organs.10,11 B cells undergo receptor editing in the bone marrow, while T cells undergo negative selection in the thymus.10,11 Although these mechanisms evolved to prevent immune responses against self-antigens, the same pathways that maintain self-tolerance may also be exploited to induce donor-specific tolerance toward alloantigens in solid organ transplantation.11
Mechanisms of peripheral tolerance take place in secondary lymphoid organs, such as the spleen and lymph nodes, as well as at sites of immunological responses (e.g., the donor organ itself).11 Therefore, autoreactive cells that escape from the primary lymphoid organs to the secondary lymphoid organs may undergo further selection via peripheral tolerance mechanisms.10,11 Some T cells may encounter moderate strength immune signals in the thymus or come into contact with interleukin-2 (IL-2) or transforming growth factor-β (TGF-β) in the periphery, causing them to develop into regulatory T cells (Tregs), which suppress immune responses.11 Peripheral tolerance may also be induced through anergy, a state of hyporesponsiveness that occurs when an immune cell recognizes its cognate antigen in the absence of the costimulatory signals required for full activation.10,11 In addition, peripheral deletion eliminates lymphocytes through activation-induced cell death following strong stimulation of their cognate antigen receptors.11
Operational tolerance refers to a graft that does not show histological signs of acute or chronic rejection despite the absence of immunosuppression for ≥1 year.8,12 While operational tolerance shares some features with true immune tolerance, it encompasses a spectrum of immunological states in which a graft may survive and maintain clinical function without immunosuppression, more clearly describing what may be observed in SOT recipients.13 Although possible, spontaneous operational tolerance is rare, highlighting the need for supportive therapies to induce or maintain immune tolerance.8,14
The role of extracorporeal photopheresis (ECP) in inducing immune tolerance
ECP is an immunomodulatory leukapheresis-based therapy that has emerged as a potential immune tolerance-promoting strategy in solid organ transplantation.2,7 Currently, ECP is well established as a second-line therapy for chronic graft-versus-host disease (GvHD) and is recommended in Europe as an adjunctive therapy for the prevention and management of heart or lung transplant rejection in adults, with evidence supporting its use in liver and kidney transplantations.15–17
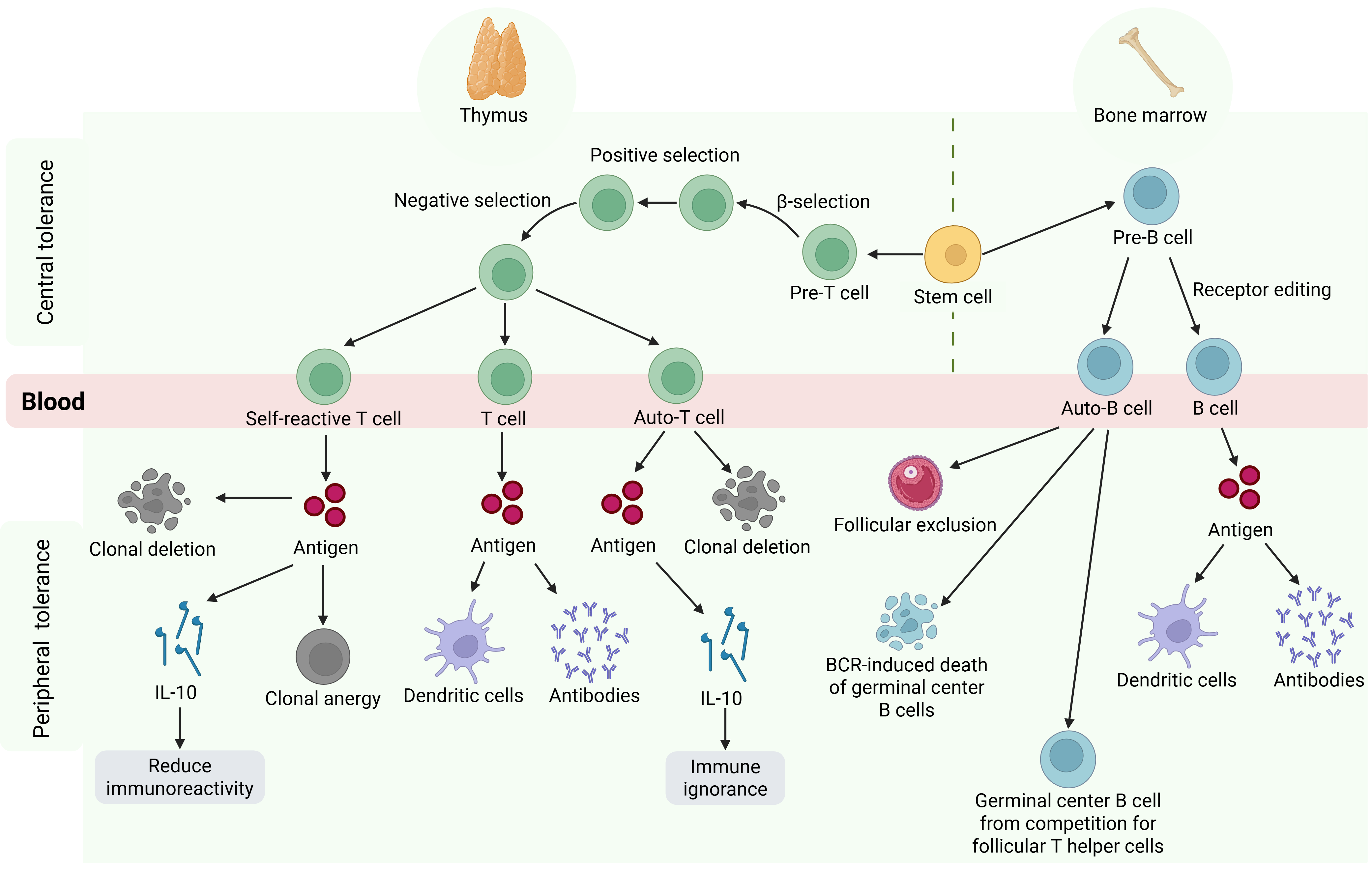
The ECP procedure involves collecting whole blood from a patient and separating leukocytes. The leukocytes are then treated with 8-methyoxypsoralen, a photosensitizing agent, and exposed to ultraviolet-A irradiation, which initiates apoptosis. The photoactivated leukocytes are then reinfused into the patient.2,18 The exact mechanism of action of ECP has not been fully elucidated; however, it is widely acknowledged that apoptotic leukocytes interact with dendritic cells in lymphoid tissue, leading to stimulation of Tregs, modification of cytokine expression from proinflammatory to anti-inflammatory profiles, and suppression of alloantigen-responding T cells (Figure 2).7 Although effects may differ depending on the baseline immune condition of the patient, it has been shown in patients with GvHD that ECP leads to a shift towards a tolerogenic immune profile.2,7
Figure 2. The proposed mechanism of immune tolerance with ECP
Clinical evidence supporting the use of prophylactic ECP for SOT rejection prevention
The volume of research into ECP as a prophylactic therapy for transplant rejection varies per organ type, with use more widely encountered in cardiothoracic transplantation compared with abdominal transplantation (Table 1).2,7 No established guideline recommendations for the use of ECP in liver or kidney transplantation currently exist, and most evidence supporting the use of ECP in this setting is limited to retrospective, single-center, and case studies.2,7,16
Table 1. Clinical evidence supporting ECP in rejection prevention and management
| Publication and study type | Transplant type and therapeutic used | Findings |
| Cardiothoracic organ transplantation | ||
Barr et al. 199819 Preliminary study | Heart ECP + standard therapy (n = 33) vs standard therapy alone (n = 27) |
|
Gökler et al. 202220 Prospective study | Heart Prophylactic ECP + low-dose immunosuppression (N = 28) |
|
Barten et al. 202318 European multicenter, retrospective study | Heart ECP + immunosuppression (N = 105) |
|
Benazzo et al. 202421 European multicenter, retrospective study | Lung ECP following azithromycin or montelukast for CLAD (N = 631) |
|
| Abdominal organ transplantation | ||
Tamain et al. 201922 Multicenter, retrospective study | Kidney ECP ± standard therapy (N = 33) |
|
Gregorini et al. 202123 Prospective, observational study | Kidney ECP + standard therapy (N = 14) |
|
Mazzoni et al. 201724 Single-center experience | Liver ECP + immunosuppression (N = 367) |
|
ACR, acute cellular rejection; AMR, antibody-mediated rejection; CLAD, chronic lung allograft dysfunction; ECP, extracorporeal photopheresis; eGFR, estimated glomerular filtration rate; HCV, hepatitis C virus; ISHLT, International Society for Heart and Lung Transplantation.
Challenges, limitations, and future directions
While ECP is recommended for the prevention of rejection following heart and lung transplant in Europe, the absence of international guidelines across organ types limits current applications.16,17 Similarly, clinical data supporting the use of ECP for rejection prevention remain limited, particularly in the abdominal transplantation setting.2,7 Future research focusing on immune tolerance-inducing therapies, such as ECP, is warranted to improve SOT outcomes and reduce or eliminate the need for lifelong systemic immunosuppression.8 Moving forward, standardized protocols and guidelines, alongside growing clinical evidence supporting the use of ECP, may increase confidence in its use for immunomodulation and the promotion of immune tolerance to prevent SOT rejection and subsequent complications.16
Conclusion
Overall, ECP represents a promising adjunctive strategy in solid organ transplantation for promoting immune tolerance through immunomodulatory rather than immunosuppressive mechanisms.7,16 However, knowledge and use of ECP in SOT rejection prophylaxis varies by organ type, with guideline recommendations and studies of ECP in cardiothoracic transplantation outweighing those in abdominal transplantation.16 Future studies are required to further understand the mechanisms of immune tolerance and to identify therapies that induce immune tolerance for rejection prophylaxis in patients undergoing solid organ transplantation.
This educational resource is independently supported by Therakos. All content is developed by SES in collaboration with an expert steering committee. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content


