All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional.
The SOT Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the SOT Hub cannot guarantee the accuracy of translated content. The SOT Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.

The SOT Hub is an independent medical education platform, supported through a founding grant from Therakos. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View solid organ transplantation content recommended for you
Rejection prevention in SOT: Immunosuppression-sparing strategies and the role of ECP
Do you know... Which of the following is not true regarding the rationale for use of ECP in SOT rejection prevention?
Solid organ transplantation is an established treatment option for patients with end-organ dysfunction that is terminal or is associated with significantly reduced quality of life (QoL).1 In 2025, 49,065 patients in the US and 7,967 patients in Europe received a solid organ transplant (SOT).2,3
Immunological mechanisms of transplant rejection
While SOT practices are continually evolving, graft loss due to immune rejection remains a common and critical complication following transplantation.1,4 The understanding of transplant rejection immunology is rooted in the self/non-self model (SNS), in which the immune system differentiates between own and foreign matter.5 However, as immunological understanding has progressed, the SNS model has not fully been able to explain transplant outcomes5, and alternative models, such as the stranger and danger models, have been developed to further explain immunological responses.6 The danger model describes how the immune system recognizes and defends against any form of cellular stress/injury, while the stranger model describes how allo-antigens trigger immune responses based on genetic differences between the SOT recipient and the donor.6 It has been further suggested that graft survival does not rely solely on the absence of immune reactions and may instead be supported by regulatory mechanisms that enable coexistence between the immune system and the graft.5
Transplant rejection is modulated via innate and adaptive immune responses, and can be classified as acute or chronic and either T-cell or B-cell mediated, although mixed-rejection types have been reported.4,7 The innate immune response is guided by neutrophils, macrophages, natural killer cells, and dendritic cells (DCs), which activate adaptive immune responses and cause graft damage through the release of reactive oxygen species and pro-inflammatory cytokines.7 The adaptive immune response depends on: T cells, which further stimulate the innate immune response, activate B cells, and cause direct damage through pro-apoptotic enzymes; and B cells, which differentiate to plasma and memory B cells and induce antibody-dependent cell-mediated cytotoxicity.6
Prevention of SOT rejection
To circumvent graft rejection, systemic, life-long immunosuppressive regimens are usually administered, including induction, maintenance, and rejection protocols, with the ultimate goal of suppressing the innate and adaptive immune responses.1 Induction therapy is initiated prior to or during the early post-operative period of transplantation and typically consists of high-dose steroids and antithymocyte globulin, alemtuzumab, or anti-interleukin-2 (IL-2) antibodies, such as basiliximab.1,4 Standard of care maintenance regimens generally involve a calcineurin inhibitor (CNI), an anti-metabolite, and corticosteroids.1,4 In the event of SOT rejection, the immunosuppressive regimen is altered to include high-dose corticosteroids and short courses of antithymocyte globulin, although augmentation of treatment depends on whether rejection is cellular or antibody-mediated.4
While immunosuppressive techniques have been effective in reducing the risk of graft rejection or death following SOT, challenges remain.4 A key complication associated with immunosuppression is the increased risk of infection, often by opportunistic pathogens such as cytomegalovirus, herpes simplex virus, and Mycobacterium tuberculosis.4 Additionally, initiating and maintaining an appropriate level of immunosuppression requires balancing graft longevity and risk mitigation, with rejection and infection associated with under- and over-suppression, respectively.8 Treatment-related adverse events are common at the time of transplantation; for example, exposure to CNIs is associated with nephrotoxicity, hypertension, dyslipidemia, and post-transplant diabetes.4,8 There is also an established link between immunosuppression and oncogenesis, with increased risk of lymphoma, skin cancer, and cervical cancer.1,4
The incidence rate and type of immunosuppressant-related complications varies per organ type, emphasising an unmet need for individualized treatment strategies and methods of minimizing the side effects of conventional immunosuppressive therapy.4,9 A possible solution is integration of immunomodulatory therapies, such as extracorporeal photopheresis (ECP), which suppress immune responses associated with graft rejection but do not induce global immunosuppression.10
ECP for SOT rejection prevention
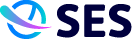
ECP involves the collection of whole blood from a patient, exposure of their leukocytes to 8-methyoxypsoralen and ultraviolet-A irradiation, then reinfusion (Figure 1).4,11 Currently, ECP is well established as a second-line therapy for the treatment of chronic graft-versus-host disease, an immune-mediated syndrome that is a major complication following allogeneic hematopoietic stem cell transplantation,12 and is recommended by the American Society for Apheresis (ASFA) for the treatment of heart transplant rejection and by the International Society for Heart and Lung Transplantation (ISHLT) for chronic or resistant acute rejection.4
Proposed mechanism of action of ECP
At present, the underlying mechanism of action of ECP is not fully understood, but it is generally accepted that immunomodulation occurs as a result of apoptotic leukocytes interacting with DCs in lymphoid tissue, leading to downstream immune regulation (Figure 1).10 The promotion of regulatory T-cell production through ECP allows immune modulation to support graft retention without inducing global immunosuppression.4
Figure 1. Procedure and mechanism of action of ECP*
Clinical evidence supporting the use of ECP in SOT
The volume of research into ECP as a prophylactic therapy for transplant rejection varies per organ type, with use more widely encountered in cardiothoracic transplantation compared with abdominal transplantation (Table 1).4,10 No established guideline recommendations for the use of ECP in liver or kidney transplantation are currently available, and most evidence supporting the use of ECP in this setting is limited to retrospective, single-center, and case studies.4,10,14
Table 1. Key results from clinical studies evaluating ECP for SOT rejection prevention
Publication and study type | Transplant type and therapeutic used | Findings |
|---|---|---|
Cardiothoracic organ transplantation | ||
Barr et al. 199815 Preliminary study | Heart ECP + standard therapy (n = 33) vs standard therapy alone (n = 27) |
|
Gökler et al. 202216 Prospective study | Heart Prophylactic ECP + low-dose immunosuppression (N = 28) |
|
Barten et al. 202311 European multicenter, retrospective study | Heart ECP + immunosuppression (N = 105) |
|
Benazzo et al. 202417 European multicenter, retrospective study | Lung ECP following azithromycin or montelukast for CLAD (N = 631) |
|
Abdominal organ transplantation | ||
Tamain et al. 201918 Multicenter, retrospective study | Kidney ECP ± standard therapy (N = 33) |
|
Gregorini et al. 202119 Prospective, observational study | Kidney ECP + standard therapy (N = 14) |
|
Mazzoni et al. 201720 Single-center experience | Liver ECP + immunosuppression (N = 367) |
|
ACR, acute cellular rejection; AMR, antibody-mediated rejection; CLAD, chronic lung allograft dysfunction; ECP, extracorporeal photopheresis; eGFR, estimated glomerular filtration rate; HCV, hepatitis C virus; ISHLT, International Society for Heart and Lung Transplantation.
Challenges, limitations, and future directions
A European review, investigating the current use and knowledge of ECP in solid organ transplantation, found that awareness of ECP as a therapeutic option varied greatly with organ type, with 63%, 57%, 69%, and 24% of clinicians reporting awareness of ECP as a treatment option for the rejection of heart, lung, kidney, and liver transplants, respectively.14 While ECP is recommended in international guidelines, such as ISHLT, for the treatment of lung and heart transplant rejection, the absence of guidelines across organ types limits application of ECP at present.4,14
Additionally, as ECP requires specialist equipment, facilities, and trained clinicians, it may not be offered by all transplant centers, making access challenging.14 If patients are then required to travel to specialist centers for treatment, financial and logistical factors may further limit access.14 Variations in global healthcare systems mean reimbursement policies differ and may not cover the full cost of ECP, further limiting availability by socioeconomic status.14
When asked about factors that may encourage the use of ECP for solid organ transplantation across organ types, European clinicians noted that more robust trial data supporting ECP for the treatment of transplant rejection and for rejection prevention, standardized protocols or guidelines, research into biomarkers to predict ECP outcomes, education on ECP, and stronger cost–benefit data would be beneficial (Table 2).14
Table 2. The percentage of European clinicians in agreement with factors which would increase the use of ECP in solid organ transplantation, per organ type*
| % of clinicians in agreement | ||||
|---|---|---|---|---|
| Factor | Heart (n = 13) | Lung (n = 8) | Kidney (n = 24) | Liver (n = 6) |
| Robust data for the use of ECP in the treatment of SOT rejection | 69 | 100 | 92 | 83 |
| Availability of standardized protocols/guidelines | 85 | 63 | 83 | 67 |
| Robust data for the use of ECP in the prevention of SOT rejection | 85 | 75 | 79 | 33 |
| Research into biomarkers to predict responses to ECP | 69 | 88 | 42 | 50 |
| Education on how to select candidates for ECP | 31 | 50 | 58 | 33 |
| Education on the mechanism of action and benefits of ECP | 38 | 13 | 58 | 50 |
| Stronger cost-benefit data | 15 | 63 | 42 | 17 |
| Robust data for the safety of ECP in solid organ transplantation | 15 | 0 | 46 | 33 |
*Adapted from Cashmore et al., in accordance with the Creative Commons Attribution (CC by 4.0) license.
ECP, extracorporeal photopheresis; SOT, solid organ transplant.
Conclusion
The immunomodulatory, rather than immunosuppressive, effects of ECP may reduce risk of infections, malignancies, and nephrotoxicity, and enable steroid sparing in patients who have undergone solid organ transplantation.10,14 However, knowledge and use of ECP in SOT rejection prophylaxis varies by organ type, with guideline recommendations and studies of ECP in cardiothoracic transplantation outweighing those in abdominal transplantation.14 Moving forward, the development of standardized protocols/guidelines and the emergence of clinical data supporting the use of ECP, particularly in abdominal organ transplantation, may improve confidence in implementing ECP for SOT rejection treatment and prophylaxis.14
This educational resource is independently supported by Therakos. All content was developed by SES in collaboration with an expert steering committee. Funders were allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content


